
Outstanding foot and ankle surgery in Sussex and London
Our orthopaedic surgeons Mr. Dirk Nowak and Mr. Dieter Nollau are internationally renowned specialists in operations for foot and ankle diseases. Contact us at The Worthing Laser & Skin Clinic in Worthing for more details.
Are foot problems mainly an issue affecting women? Women have more vulnerable supporting and connective tissue. This, coupled with hormonal influences and exposure to pregnancy and childbirth, as well as the use of high-heeled shoes, is a main cause of the problems. Style and design in shoe fashion unfortunately gives no consideration to foot health. The result is about 85% of women over 40 suffer from major foot problems.
But is it only women’s feet that are particularly vulnerable? No. Certain sports promote changes to the feet. Football players suffer problems due to the extreme weight-bearing on their standing leg. With sports women it is mainly tournament, ballet dancers and tennis players who suffer problems. Of course all people whose occupations involve standing for hours on end are also at risk, whether men or women.
How does a bunion develop? The bunion (Hallux valgus) is caused by a splay and flat foot. The joint head of the first metatarsal gradually emerges. The bale is not as often suspected as too much bone (ganglion). If the big toe bends laterally, the neighbouring toes lack space. The pressure between the toes increases. The consequences are calluses, under and over-crossing toes and finally claw and hammer toes. The result is called a “complex fore foot deformity” and such a foot will not fit into any normal shoe and every step is excruciating.
What can you do to prevent a bunion? If a bunion exists already, an operation is the only option to restore the original shape and function of the metatarsal joint. There are very gentle and careful surgical methods available today.
Could insoles solve the problem? They can form the first line of defence but insoles are only effective in early stages as they provide relief to an already damaged foot.
And how about foot exercises to combat foot pain? Basically, every workout of the muscles that support the lateral and longitudinal arch is useful because the muscles are extremely stretched by the lesion of the foot and so wear out. Targeted exercises for the foot include trying out different gaits, such as only walking on the toes then on the heels, changing to walking on the inside and outside edges of the foot. You can stand your foot on the ground and pull the toes to the front or leave a towel on the floor and claw it with the toes. You can spread the big toe inward, then spread all toes and try a “playing piano” movement with the toes.

When is an operation the only option? If, after lowering of the longitudinal and/or transverse arch, hammer toes or bunions have emerged, the affected foot will continue to get worse. The new, gentle surgical methods are possible even at a young age because no functioning joints are destroyed.
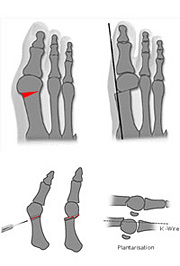
What happens during the procedure?The most successful and most gentle micro-invasive surgical technique for the patient is the displacement of the first metatarsal bone, known as the Boesch technique. The incision is only 5 to 10 millimetres, followed by a very gentle bone conversion and reorientation. In addition, there are other osteotomy procedures available, depending on the diagnosis. In some operations the longitudinal and square arch can be erected simultaneously. Thus, the foot gets back to an optimum function.
Is it ever too late for an operation? No, but most sufferers come to see the doctor far too late and usually only when the pain of wearing normal shoes has become unbearable and/or impossible. However, the pain is the last signal, marking the end of a change in the foot, which took over 10 to 15 years to complete and this should not have to be tolerated.
What causes this raging pain? The bunion (Hallux valgus) affects the performance of the foot. The function of the first fore foot beam is weakened – this is the part of the foot from the big toe to the first metatarsal. As a result, the rest of the foot bears more and more weight when walking and rolling, putting stress on the foot. The pressure on the sole of the foot increases, calluses grow and pain is the result. The foot has fallen out of balance. At this stage, the joint at the big toe dislocates, the capsule gets affected and tendons shrink – all in all an horrific scenario for the foot.
Is it more difficult to operate on a deformed foot? Yes, because the position of the joints are usually very fixed and rigid. Damage and wear and tear are well advanced. Nevertheless, almost every complex fore foot deformity can be corrected with the new, gentle surgical methods.
What happens after the operation? The procedure is performed as an outpatient and the patient leaves the clinic on foot, immediately able to put full weight on their foot/feet. A wire is introduced into the foot as a kind of internal splint and stabilises the foot. The wire will be removed pain free after four weeks. The patient will have to wear special sandals for about 6 weeks to protect the operated foot/feet.
What happens when both feet are damaged? In 90 per cent of cases, both feet are operated on at the same time, simply because the patient can walk immediately after the operation. The patient is therefore self-sufficient and not dependent on post-op care. Hours of walking and standing in the early stages after the operation is not advised, however, after weight-bearing intervals the foot should be rested and cooled.
How long does the healing process after surgery take? After four weeks the wire is removed you will be asked to wear the Darco bandage for another 2 weeks to support the foot further. After that you can start wearing wider shoes and gradually get back into your nice shoes with heels. The bones will heal completely over the next 8 weeks. Should swelling occur, lymphatic drainage and cooling will help.
What are the risks of foot surgery? Due to the micro-invasive surgical method, which does not require large incisions, the risks are relatively minimal. In the last 10 years, over 8,500 patients have had the procedure and did not experience any major complications.
How successful is this operation? As part of a multi-centre post-operation study, involving American results for the methods of refurbishment and conversion of the foot bones in minimally invasive techniques, a high success rate of good and excellent results was found in patients who had had the intervention more than six years previously .
Are the feet bigger after surgery? The feet reach their original size again. The bunion leading to the surgery will have changed the shape of the foot and in a few cases, the operated foot will be slightly narrower as before.
What rehabilitation measures are necessary after surgery? A targeted physiotherapy is only required in exceptional cases. In general, constant movement of the toes, lymphatic drainage, as well as spreading and stretching exercises, is enough to strengthen the muscles. When walking, you should pay particular attention to the rolling of the feet so that the function of the metatarsophalangeal joints and the erected arch are back to normal.
How long until the foot is fully recovered? After about 7 weeks, the foot is fully stabilised so the patient can take up the usual activities at work, home and sports again. Considering the foot had been deformed for a decade or more, this course of treatment is extremely short.


What is osteoarthritis in the foot? The cartilage layer acts as a shock absorber in all joints. Accidents and wear fray the cartilage surface gradually destroying it. If the arthritis progresses, the bone is exposed and unprotected.This results in a lot of pain and stiffness in the affected joints such as shoulders, knees, hips, and feet too. The ankle will gradually get stiff, up rolling on your foot will be impossible and every step will become excruciating.
How is osteoarthritis treated in the foot? For a long time there have been no effective treatment options. Previously, the foot was often stiffened. For younger people cartilage cells grown in the laboratory can be inserted into the joint to regenerate the damaged cartilage. However, these are very expensive procedures which always go hand in hand with a long recuperation period for the respective joint. If the damage is very advanced, the affected joint can be replaced by a full prostheses similar to the one used in a hip replacement.
Reasons against a prosthesis? None, but it should be the very last option for the treatment of osteoarthritis because a joint replacement, whether in a hip or a foot has a limited life. The life expectation is between 15 and 20 years which is one of the reasons to try to postpone the operation for as long as possible.
But if it’s too early for a prosthesis, which can be done about it? An innovative alternative from the U.S has been on the market for the last 10 years – a soft implant made of water-storing plastic, is used in the affected metatarsal joint. This hydro gel implant is made of the same base material substance as used for the production of soft contact lenses.
How does the implant work? The human cartilage acts like a shock absorber in the joints. The implant takes over the original function of the cartilage and acts as a sliding buffer between the two articular surfaces. The 10mm small implant is inserted during minimally invasive surgery. The method is suitable for osteoarthritis of the big toe base joint, only if one side of the joint is still intact. A study for the Food and Drug Association (FDA) in the USA on 76 patients, with a follow-up period of over four years post-operatively, resulted in an improvement of the main complaints such as pain and function by up to 282%.
What advantages does this method have?
The foot can weight bear immediately, and after the procedure normal foot function is quickly restored. There is an almost painless and very short healing period and the implant is wear-resistant and could work for a lifetime. It is also allergy-free and there are no incompatibility issues.
What other alternatives do affected patients have?
In many cases, reinforcement (stiffening of the joint) is recommended in the early stages. This is an irreversible procedure that needs to be well thought through. Nevertheless, a successful stiffening will make you pain free. Under the American influence Hemi-caps are increasingly being used as partial replacement and over-capping of damaged parts of the joint. However parts of the joints are being completely removed. The patient concerned will have to seek advice from their specialist to select the most appropriate operation.
The clinic has the latest and most modern approach of foot related injuries and we welcome people from all over the Country, including London, Brighton, Southampton, Bournemouth, Birmingham, Manchester, and Newcastle etc. Patients receive first class care and advice in a calm and professional manner.